MedixMAB Tumour Markers
Tumour markers are a diverse group of proteins and other molecules that are secreted by cancer cells, or normal cells, in response to tumours and related conditions. Most tumour markers are also produced under noncancerous circumstances; their expression, however, is upregulated during cancer. Determining the presence and concentration of tumour markers in bodily fluids thus supports early tumour detection and can aid treatment follow-up and efficient choice of therapy.
Improved cancer management will become increasingly important in the future, as patients continue to live longer and cancers become more and more prevalent. Various tumour markers are currently used in clinical practice to monitor treatment success, characterize disease, as well as to support cancer diagnosis and detection. An elevated tumour marker level can also result from benign conditions. On the other hand, cancer can be present in the absence of typical tumour markers.
In practice, tumour marker immunoassays are therefore often combined with other tests to ensure reliable results. For example, immunoassays for human prostate-specific antigen (PSA) are commonly used to evaluate the pathological grade of prostate cancer and to aid early prostate cancer detection. As PSA overexpression is also related to some noncancerous conditions, measurements for both the total PSA concentration and the free form of PSA are often combined to improve cancer-specificity. Another example is carcinoembryonic antigen (CEA). Immunoassay can be a useful tool in predicting the therapeutic effect, progression, and prognosis of the several cancers.
CA125
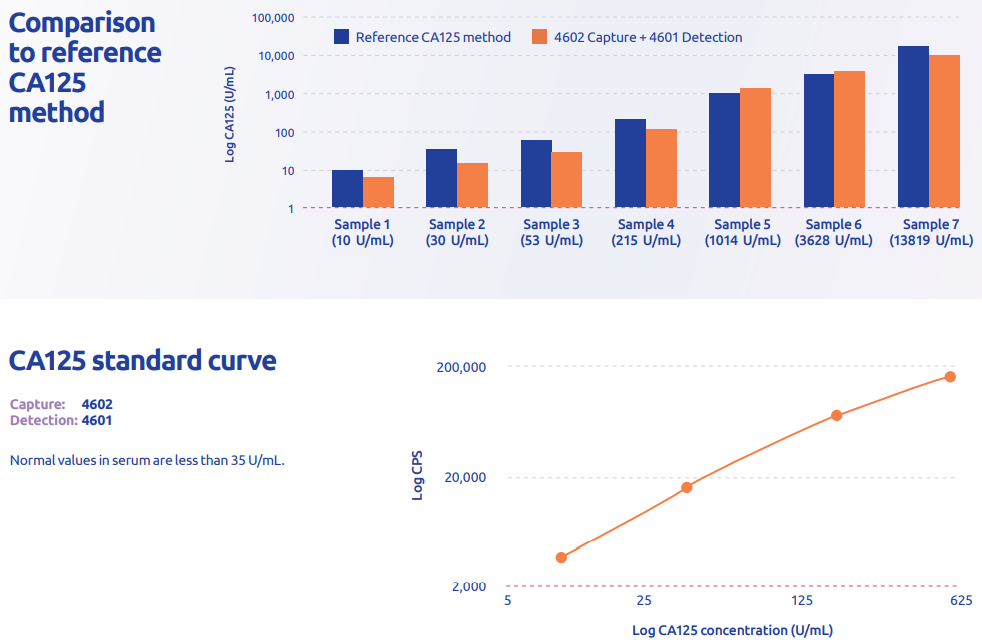
Cancer antigen 125 (CA125) is a peptide epitope produced by the mucin 16 (MUC16) gene. CA125 was among the first tumour biomarkers discovered, defined by the binding of murine monoclonal antibody OC125. Other CA125 antibodies have subsequently been developed, and they are classified as OC125-like (group A), M11-like (group B), or OV197 (C). Epithelial cells in the respiratory tract, female reproductive tract, and cornea express CA125 on their membranes, from where it can be cleaved and released.
CA125 is the most widely used serum biomarker to monitor epithelial ovarian cancer; it is overexpressed in 80 percent of all disease cases, and in 90 percent of patients who have stage III/IV disease. Currently, CA125 is used to monitor ovarian cancer treatment and detect residual or recurrent disease, as well as for the differential diagnosis of pelvic masses. To improve specificity and sensitivity, assays for CA125 and HE4 (another marker for ovarian cancer) are often combined. Medix Biochemica offers two monoclonal antibodies (4601 and 4602) for the detection of CA125. Based on their specificities, antibody 4601 is OC125-like and 4602 M11-like.
| CA125 antibody | SKU | Conc. (mg/mL) | Shelf life (months at +2–8°C) | Subclass |
|---|---|---|---|---|
| 4601 | 100598 | 5 | 12 | IgG1 |
| 4602 | 100628 | 5 | 12 | IgG1 |
CEA
Carcinoembryonic antigen (CEA), also known as CD66e and CEACAM5, is a 180–200 kDa glycoprotein involved in cell adhesion. It is normally produced in the fetal digestive tract, but since the production is repressed after birth, CEA levels are usually very low in normal adult colon and blood. Elevated CEA serum levels are, however, raised by various types of carcinomas, including colorectal, lung, and breast cancer. Therefore, CEA has been widely used as a broad-spectrum tumour marker. CEA is not specific to any cancer type, but its concentrations in blood may predict the therapeutic effect, progression, and prognosis of the disease.
CEA is most widely used in detecting gastrointestinal cancers, especially colorectal cancer. Several organizations recommend the measurement of both preoperative and postoperative levels of CEA in patients with colorectal cancer. Furthermore, CEA is suggested as the marker of choice for monitoring the efficacy of systemic therapy against metastatic disease. For patients with lung cancer, serum levels of CEA may carry prognostic and predictive information of risk of recurrence. Similarly, elevated CEA levels serve as an independent predictor of decreased survival in pancreatic adenocarcinoma.
Increased CEA levels are also associated with a number of benign conditions, such as inflammatory bowel disease, liver cirrhosis, pancreatitis, and smoking. Along with CEA, members of the CEA-related gene family include cross-reacting antigens, such as CD66c (also called NCA, NCA50/90, and CEACAM6), CD66a (also called BGP, BGP-1, and CEACAM1), and meconium CEA (also called NCA-2).These CEA-like proteins share common epitopes with CEA, but they also have protein domains distinctive to each molecule.
Medix Biochemica offers five different monoclonal antibodies for CEA detection. Two of them are specific to CEA (5909 and 5910) with no known cross-reactivity to other CEA-like molecules. Of the three remaining antibodies, two cross-react with NCA-2 (5911 and 5912) and one has negligible cross-reactivity to both NCA and NCA-2 (5905).
| CEA antibody | SKU | Conc. (mg/mL) | Shelf life (months at +2–8°C) | Subclass | Applications |
|---|---|---|---|---|---|
| 5905 | 100044 | 1 | 36 | IgG1 | ELISA, CLIA |
| 5909 | 100428 | 5 | 36 | IgG1 | ELISA, CLIA |
| 5910 | 100047 | 5 | 36 | IgG1 | ELISA, CLIA |
| 5911 | 100048 | 1 | 24 | IgG1 | ELISA, CLIA |
| 5912 | 100049 | 1 | 36 | IgG1 | ELISA, CLIA |
| Detection | ||||||
|---|---|---|---|---|---|---|
| 5905 | 5909 | 5910 | 5911 | 5912 | ||
| Capture | 5905 | - | - | - | - | - |
| 5909 | + | - | + | - | - | |
| 5910 | - | + | - | - | + | |
| 5911 | - | - | - | - | - | |
| 5912 | - | - | + | - | - | |
| CEA antibody | Affinity constant,KA |
|---|---|
| 5905 | 5 x 1010 1/M |
| 5909 | 3 x 1010 1/M |
| 5910 | 1 x 1011 1/M |
| 5911 | 1.5 x 1010 1/M |
| 5912 | 4 x 109 1/M |
PSA
Prostate-specific antigen (PSA) is a glycoprotein produced by the epithelial cells of the prostate gland. PSA belongs to the kallikrein protein family, and has chymotrypsin-like protease activity. It is secreted into seminal plasma, where it catalyzes the liquefaction of the seminal coagulation formed immediately after ejaculation.
Small quantities of PSA are found in the serum of men with healthy prostate, but elevated serum PSA levels indicate the presence of prostate cancer or other prostate disorders. PSA is the most widely used marker for early detection of prostate cancer. Increased concentrations of serum PSA are associated with elevated prostate cancer risk, a higher pathological grade of the cancer, and a higher risk of metastatic disease. Since the 1980s, PSA screening has significantly improved prostate cancer survival rates and the overall disease management.
PSA is organ specific, and expressed only in the prostate. However, it is not a cancer-specific biomarker, since elevated PSA levels may also reflect benign conditions. Thus, there is an ongoing debate over PSA-based screening and whether it will lead to overdiagnosis and overtreatment. The cancer-specificity of PSA-based screening can be improved by measuring the free form PSA (fPSA) and comparing it to the total PSA (tPSA), which consists of fPSA and complex PSA attached to serum protease inhibitors. fPSA accounts for 5-35% of tPSA. Low fPSA/tPSA ratio is associated with cancer, whereas high fPSA/tPSA indicates the presence of nonmalignant conditions.
Medix Biochemica offers four different anti-PSA monoclonal antibodies (8301, 8311, 8312, and 8313). The selection includes two antibodies that recognize both complex PSA and fPSA (8301 and 8311). Antibody 8312 has a binding profile that favors fPSA, with 15% cross-reactivity with PSA-ACT (antichymotrypsin) complex; antibody 8313 is fPSA-specific without cross-reactivity with the complex form.
Anti-human PSA monoclonal antibodies
| PSA antibody | SKU | Conc. (mg/mL) | Shelf life (months at +2–8°C) | Subclass | Applications tested |
|---|---|---|---|---|---|
| 8301 | 100102 | 5 | 36 | IgG1 | ELISA |
| 8311 | 100103 | 1 | 36 | IgG2a | ELISA |
| 8312 | 100139 | 5 | 36 | IgG1 | ELISA |
| 8313 (free) | 100488 | 5 | 18 | IgG1 | ELISA |
| Detection | |||||
|---|---|---|---|---|---|
| 8301 | 8311 | 8312 | 8313 | ||
| Capture | 8301 | - | + | + | + |
| 8311 | - | - | - | + | |
| 8312 | - | - | - | + | |
| 8313 | - | - | - | - | |
| PSA antibody | Association rate constant, kon | Dissociation rate constant, kof | Affinity constant,KA |
|---|---|---|---|
| 8301 | N/D | N/D | 1 x 1011 1/M |
| 8311 | N/D | N/D | 1 x 1010 1/M |
| 8312 | N/D | N/D | 3 x 109 1/M |
| 8313 (free) | 2.0 x 106 1/Ms | 1.5 x 10-5 1/s | KA = 1.3 x 1011 1/M, KD = 7.5 x 10-12 M (= 7.5 pM) |